|
Answer
Tricyclic antidepressant
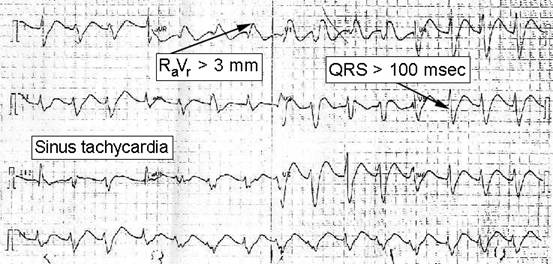
poisoning: This patient has a typical presentation for
tricyclic antidepressant overdose, given his altered
mental status, sinus tachycardia with a prolonged QRS
interval, rightward axis, and seizure. Tricyclic
antidepressants (TCAs) are prescribed less commonly
now than in the past to treat depressive disorders
because of the availability of newer antidepressants,
such as the selective serotonin reuptake inhibitors (SSRIs),
which have an improved safety profile. However, TCAs
continue to be widely used in the management of
chronic pain, selected psychiatric illnesses (eg,
obsessive compulsive disorder, eating disorders), and
in enuresis. As a class, they are responsible for more
drug-related deaths than any other medications.
Tricyclic antidepressants have a narrow therapeutic
index and can cause toxicity, even at therapeutic
doses. The toxicity is related to their mechanism of
action. These drugs block not only fast sodium
channels in myocytes but also alpha-adrenergic
receptors and amine uptake (eg, norepinephrine), and
they competitively inhibit muscarinic, histaminic, and
gamma-aminobutyric acid (GABA)–A receptors.
Patient presentations vary substantially and can range
from that of mild antimuscarinic symptoms (eg, dry
mucous membranes, dry skin, sinus tachycardia,
depressed mental status, urinary retention) to severe
and life-threatening complications (eg, cardiac [supraventricular
or ventricular tachycardia, hypotension], neurologic
[confusion, seizures, coma], and pulmonary
[respiratory depression, adult respiratory distress
syndrome, pulmonary edema] events). Life-threatening
complications usually occur within 6 h of ingestion.
Secondary complications include aspiration pneumonia,
hyperthermia, rhabdomyolysis, and anoxic
encephalopathy.
Tricyclic antidepressant toxicity should be suspected
in any patient presenting in the appropriate clinical
setting. Appropriate evaluation and start of therapy
should not be withheld while one awaits the results of
toxicologic screening to confirm the diagnosis. ECG
abnormalities are useful in identifying patients at
risk for life-threatening complications. Although
sinus tachycardia is the most common ECG abnormality,
it is only 70% sensitive for the symptomatic
presentation of life-threatening complications.
Boehnert and Lovejoy reported that QRS intervals of
100 ms or longer were predictive of seizures and
ventricular arrhythmias. Liebelt et al found that the
height of the R wave in lead aVR from the baseline PQ
segment (RaVR) of 3 mm or more was
predictive of life-threatening adverse outcomes
(sensitivity = 81%, positive predictive value [PPV] =
43%); for this purpose, RaVR was better
than a QRS interval of 0.010 s (sensitivity = 82%, PPV
= 35%).
Life-threatening complications determine the
treatments for tricyclic antidepressant toxicity.
Whereas patients with a mildly anticholinergic
response may do well with several hours of observation
and discharge, the patient with ECG changes described
above, hypotension, ventricular dysrhythmias,
seizures, or coma requires immediate aggressive
therapy. Cardiotoxic treatment is focused on reversing
competitive antagonism of the fast sodium channels by
giving a 1- to 2-mEq/kg bolus of sodium bicarbonate
(NaHCO3) followed by a continuous infusion (typically
2-3 ampules of NaHCO3 mixed into 1 L D5W).
This is administered at 2 times maintenance rate for
intravenous fluid. The desired serum pH is 7.5-7.55 to
alkalinize the serum. Hypokalemia is an expected
result of NaHCO3 therapy and should be
remedied by adding potassium to the fluid after urine
output is observed.
Standard Advanced Cardiac Life Support (ACLS)
protocols for ventricular tachydysrhythmias should be
followed, though early administration of NaHCO3
and class IB antidysrhythmics (eg, lidocaine) should
be considered.
Class
IA
or IC antidysrhythmics should be avoided, as should
class III agents (eg, beta-blockers, calcium channel
blockers). Hypotension can initially be treated with
aggressive administration of intravenous fluids.
Refractory cases may require vasoactive agents, such
as norepinephrine or dopamine (norepinephrine is less
effective than dopamine because of the patients'
depleted catecholamine stores). CNS toxicity is
typically managed with benzodiazepines as first-line
treatment for seizures. Barbiturates (eg,
phenobarbital) or anesthetics may be used for
refractory seizures.
For more information on TCA toxicity, see the
eMedicine article Toxicity,
Tricyclic Antidepressant (within the Pediatrics
specialty) and Toxicity,
Cyclic Antidepressants (within the Emergency
Medicine specialty).
References
- Liebelt
EL, Francis PD, Woolf A: ECG lead aVR versus QRS
interval in predicting seizures and arrhythmias in
acute tricyclic antidepressant toxicity. Ann
Emerg Med 1995: 26(2): 195-201.
- Boehnert
MK, Lovejoy FH: Value of the QRS duration versus
the serum drug level in predicting seizures and
ventricular arrhythmias after an acute overdose of
tricyclic antidepressants. N Engl J Med
1985;313:474-479.
- Litovitz
TL, Klein-Schwartz W, Rodgers G, et al: 2001
Annual report of the American Association of
Poison Control Centers Toxic Exposure Surveillance
System. Am J Emerg Med
2002;20(5):391-452.
- Tintinalli
JE, Kelen G, Stapczynski J: Emergency Medicine: A
Comprehensive Study Guide. 6th ed.
New York
: McGraw-Hill Professional; 2004.
|





 DISCLAIMER:
This website is designed primarily for use by qualified
physicians and other medical professionals. The
information provided here is for educational and
informational purposes only. It is not guaranteed to be
correct and should NOT be considered as a substitute for
the advice of an appropriately qualified expert. In no way
should the information on this site be considered as
offering advice on patient care decisions or establishment
of a patient-physician relationship.
DISCLAIMER:
This website is designed primarily for use by qualified
physicians and other medical professionals. The
information provided here is for educational and
informational purposes only. It is not guaranteed to be
correct and should NOT be considered as a substitute for
the advice of an appropriately qualified expert. In no way
should the information on this site be considered as
offering advice on patient care decisions or establishment
of a patient-physician relationship.